Utah Governor Spencer Cox (left) and logging executive and USFS Chief Tom Schultz (right) sign a partnership agreement.
Late Tuesday afternoon, with the subtlety of a wrecking ball and the morality of a foreclosure notice, the Trump administration announced the most devastating attack on the U.S. Forest Service in the agency’s 121-year history. Not a budget cut. Not a policy shift. Not a “reorganization.” An execution.
They’re ripping the headquarters out of Washington and shipping it to Salt Lake City, Utah — the beating heart of the anti-public-lands movement in America. They’re shuttering every single one of the nine regional offices that have governed this agency since Gifford Pinchot built the system over a century ago — and with them, the career professionals who spent entire lifetimes earning the expertise and the authority to push back when politicians came calling with bad ideas and worse motives. They’re destroying more than fifty research facilities across thirty-one states, labs that house decades of irreplaceable long-term science, the kind you literally cannot restart once it’s gone. And they’re replacing all of it — the offices, the scientists, the institutional knowledge, the professional independence — with fifteen political appointees called “state directors,” embedded in state capitals alongside the very governors, legislators, and industry lobbyists who have spent their careers demanding that the Forest Service log more, protect less, and get out of the way.
One hundred and ninety-three million acres of your national forests. An area larger than Texas. The largest public land agency in the country. Just handed, on a silver platter, to the people who’ve spent their entire careers trying to destroy it.
And they did it with a press release on a Tuesday.
Upgrade to Paid
Let me be very clear about what’s happening here, because the press release is designed to make your eyes glaze over. It’s written in the dead language of bureaucratic euphemism — “mission delivery,” “state-based organizational model,” “operational service centers” — and that’s the point. They want you bored. They want you to think this is an org chart shuffle. They want you to read the word “streamlining” and move on with your day.
Don’t.
What this actually is, stripped of the Orwellian window dressing, is the largest forced purge of a federal land management agency in American history. It dwarfs anything that’s come before. The BLM headquarters move in Trump’s first term — widely understood, even then, as a deliberate gutting of the agency — involved a few hundred positions. This involves thousands. That one closed zero regional offices. This one closes all ten. That one touched one agency’s headquarters. This one dismantles the headquarters, collapses the regional structure, and wipes out the scientific backbone of the largest forestry organization on Earth.
The BLM move was a knife in the dark. This is a chainsaw in broad daylight. And just like the BLM move, it will work exactly as designed. Because we know what happens when you tell career public servants to uproot their families and move across the country on six months’ notice. We have the data. We watched it happen in real time.
Of 328 BLM positions ordered to relocate, 287 employees left the agency. Only 41 moved at all — scattered across various western offices. And only three — three human beings — actually relocated to the new “headquarters” in Grand Junction. The agency lost 87% of its Washington-based workforce. Decades of institutional knowledge, scientific expertise, and legal acumen walked out the door and never came back.
That wasn’t an accident. That was the plan. And the plan worked so well they’re doing it again at twenty times the scale.
Because the people who leave won’t be random. They’ll be the lifers. The scientists. The ones with thirty years of field experience who know what a logging plan will do to a watershed before anyone runs a model. The ones who know the law cold, who know where the bodies are buried, who have the institutional authority and the backbone to say “no” when a politician calls and demands more timber sales. Those are the people who can’t uproot their lives. Those are the people who will retire, or resign, or take jobs in the private sector.
And those are exactly the people this administration wants gone.
Because once they’re gone, you replace them. With loyalists. With industry allies. With people who have never set foot in a national forest but know exactly whose phone calls to return. You don’t need to fire anyone. You just announce a “move” and let attrition do the killing for you.
Then you fill the vacancies with your own people and pretend the agency still exists.
Of all the places on this Earth to send the agency that manages America’s national forests, they chose Salt Lake City, Utah.
Coincidence?
No.
Utah. The state that is, right now, at this very moment, suing the federal government to seize 18.5 million acres of your public land. A case engineered from the start to reach a sympathetic Supreme Court and detonate 150 years of settled public land law.
Utah. The state whose governor, Spencer Cox, just weeks ago signed a deal with this same Forest Service Chief — the former logging executive — giving Utah de facto control over Forest Service operations on eight million acres of national forest. A “partnership” we called out at the time for exactly what it was: a dry run for transfer. Control without ownership. The first step in a playbook designed to embed the state in federal decision-making so deeply that the line between federal and state management disappears, and when the inevitable push for full transfer comes, the argument writes itself: “We’re already managing it. Why shouldn’t we own it?”
Utah. The state that produced Mike Lee — the rat in the walls of Congress, the most dangerous anti-public-lands politician in modern American history — a man who has spent his entire miserable career trying to sell your national parks, gut the Wilderness Act, auction off BLM land to developers, and dismantle every protection standing between your forests and the industries that want to devour them. And if you think Mike Lee didn’t have his fingerprints all over this decision, I have a bridge over the Colorado River to sell you.
Utah. The state that has been ground zero for the anti-public-lands movement for as long as the movement has existed. A hotbed of Sagebrush Rebellion ideology, where the political class has spent decades trying every conceivable legal, legislative, and administrative maneuver to wrest federal land out of public hands and into the grip of state politicians and their industry patrons.
And now the United States government is handing them the headquarters of the agency that manages 193 million acres of national forest.
In the USDA’s press release, Utah Governor Spencer Cox calls this “a big win for Utah.”
Yes. Obviously.
And of course he’s in the release — when you’re effectively calling the shots, you tend to get top billing at the Forest Service.
It’s the biggest win Utah’s anti-public-lands machine has ever secured — bigger than Bears Ears, bigger than the Forest Service “partnership,” bigger than anything Mike Lee has managed to slither through Congress.
Because this one didn’t need Congress. This one didn’t need the courts. This one just needed a press release and a compliant logging executive with a title that says “Chief” on it.
I need to stop here because this part will make your blood boil.
Forest Service Chief Tom Schultz — a logging executive, installed by this administration to oversee the dismemberment of the agency he now claims to lead — had the gall, the sheer sickening audacity, to say this in the press release:
“I’m honored to help guide this new chapter for the Forest Service, following the vision set forth by President Theodore Roosevelt and Gifford Pinchot more than a century ago.”
Let that sink in.
Theodore Roosevelt created the national forests to protect them from exactly the kind of industrial plunder this administration is enabling. Gifford Pinchot built the Forest Service from scratch, brick by brick, to ensure that America’s forests would be managed by trained professionals in the public interest — not by political appointees serving the timber industry from a satellite office in the state that wants to own those forests.
Roosevelt fought the robber barons. Pinchot fought the timber trusts. They built this agency as a shield for the American public against the exact forces that are now being handed the keys.
And Tom Schultz — a man who made his career cutting trees for profit before being plucked from the industry to run the agency that’s supposed to regulate it — invokes their names while dismantling their life’s work.
It’s vile.
Roosevelt would have run this man out of Washington on a rail. Pinchot would have fought this tooth and nail with every ounce of breath in him. And both of them would be sickened — not just by the decision, but by the grinning cowardice of a political appointee who uses their legacy as a fig leaf while gutting everything they fought to build.
If the headquarters move is the gunshot, the destruction of the research program is the burial.
More than fifty research and development facilities across thirty-one states. Gone. Consolidated into a single location in Fort Collins, Colorado. And “consolidated” is doing a lot of heavy lifting in that sentence, because what it actually means is that decades of place-based, long-term ecological research — the kind that literally cannot exist anywhere else because it depends on specific forests, specific watersheds, specific ecosystems studied over generations — will be snuffed out.
You cannot move a thirty-year watershed study. You cannot relocate a decades-long old-growth monitoring program. You cannot box up a forest and ship it to Colorado. When these facilities close, the experiments die. The datasets end. The partnerships with universities that took generations to build collapse. And the institutional knowledge of the scientists who ran those programs walks out the door, because the administration damn well knows most of them won’t follow a forced relocation to a single consolidated office that has nothing to do with the ecosystems they’ve spent their careers studying.
This is the most respected forestry research program on the planet. It’s the reason we understand wildfire behavior, forest disease, watershed health, carbon storage, old-growth ecology, and climate adaptation. It’s the scientific backbone that every responsible land management decision depends on. It’s the envy of land managers across the world.
And they’re destroying it. Not because it’s expensive — the entire research budget is a rounding error. Not because it’s inefficient — decentralized, place-based research is the only kind of forest science that works. They’re destroying it because science is an obstacle.
Because a scientist who says “you can’t log that watershed without destroying it” is inconvenient. A researcher who publishes data showing that a timber sale will wipe out a salmon run is a problem. A lab that documents the damage from mining runoff or road-building or clear-cutting is an enemy.
And enemies get eliminated.
Once the science is gone, there’s nobody left to flag the damage. Nobody left to say “this will destroy this stream” or “this species can’t survive this level of harvest.” The unprecedented mandatory logging quotas from the reconciliation bill can proceed without anyone left who has the data, the authority, or the institutional standing to object. The timber industry gets its clearcuts. The mining companies get their access roads. And the next time someone asks “what will this do to the forest?” the answer will be silence, because the people who knew are gone and the studies that would have told us were terminated by press release on a Tuesday in March.
We’ve been writing about this for over a year. We’ve been called alarmist. We’ve been told “that’s not going to happen.”
Here’s the playbook, one more time, because it’s no longer a prediction. It’s a live feed:
Step 1: Starve the land agencies of funding, staff, expertise, and authority. Done. This administration gutted more than 25% of land management agency staff. It proposed a budget that slashed the Forest Service by a third. It tried to eliminate all Forest Service research funding.
Step 2: Break the agency’s ability to function. Done. Mass firings. Deferred resignations. DOGE operatives embedded inside the agency. Psychological warfare campaigns designed to demoralize career employees into quitting.
Step 3: Point to the dysfunction you engineered and declare the institution a failure. Done. The press release itself does this, citing “decades of mismanagement and costly deferred maintenance” — problems created by the very people now using them as justification for demolition.
Step 4: Reorganize the broken agency into something that serves your interests, not the public’s. Happening right now. Today. On your screen. With a press release that uses the words “common sense” five times.
Step 5: Hand the pieces to your allies in state government and industry. Also happening right now. The headquarters goes to Utah. State directors answer to state politicians. The research that would have documented the damage: gone. The career professionals who would have resisted: purged through “relocation.”
And there is Step 6, the one they haven’t announced yet but that every single move in this sequence is building toward:
Step 6: Transfer the land.
Because once you’ve moved the headquarters to the state that wants to own the forests, installed state-aligned political appointees as managers, destroyed the independent science, eliminated the institutional capacity to resist, and created a structure where state governments are functionally running federal forests already — the argument for formal transfer becomes very, very easy.
“We’re already managing it. Why should Washington own it?”
That’s the endgame. And after today, the path to it has never been shorter.
Zoom out. Look at the mosaic. All of it. Everything that’s happened in the last fourteen months:
A logging executive installed as Forest Service Chief. An oil governor running Interior. Steve Pearce, a man who believes Theodore Roosevelt was wrong to create national parks and forests, nominated to run the BLM. NEPA dismantled. The Endangered Species Act under siege. The Roadless Rule rescinded. Alaska’s wildlands opened to industry. Mandatory logging quotas signed into law. The God Squad convened for the first time in thirty years to override endangered species protections for oil drilling. Utah’s governor cutting a deal for control of your national forests. Utah suing for 18.5 million acres of your BLM land. Russ Fulcher circulating letters in Idaho preparing counties for federal land transfer. Mike Lee hiding poison pills in must-pass bills trying to sell your lands.
And now this. The crown jewel. The big one.
The agency that manages 193 million acres of your forests — relocated to the state that wants to own them, stripped of its science, stripped of its regional expertise, stripped of its institutional independence, and reorganized into a structure purpose-built for political compliance.
Anyone who still thinks these are unrelated events, disconnected policy decisions made by different people at different times for different reasons, is in willful denial. This is a coordinated demolition of federal land stewardship in America. Every piece connects. Every move advances the same goal: transferring control of your public lands from professional public servants accountable to you to political operatives accountable to the extraction industry.
The Forest Service was the last major federal land agency that still had the institutional muscle to resist. It had the scientists. It had the regional foresters. It had the culture, imperfect as it was, that still believed forests belonged to the public.
After today, that agency no longer exists.
There will still be people wearing the shield. There will still be an org chart and a budget line. But the Forest Service that Gifford Pinchot built — the institution that pioneered the radical idea that America’s forests are not timber inventory to be liquidated but a public trust to be stewarded — was killed today.
And they did it without a single vote in Congress.
Call your senators. Call your representative. Not next week or later. Now.
Tell them this is not a reorganization — it’s the destruction of a federal agency by executive fiat and that Congress must intervene. Tell them to block all funding for this relocation and restructuring until the full implications have been studied, debated, and voted on by the people’s elected representatives.
Tell them you know what happened to the BLM. Tell them 87% staff loss is not efficiency. Tell them that three people showing up to Grand Junction is not “moving closer to the land.” Tell them that if they allow this to proceed, the Forest Service will suffer the same fate at twenty times the scale, and the blood will be on their hands.
Tell them you know the endgame. Tell them this is the on-ramp to land transfer. Tell them that handing the headquarters to Utah while Utah is actively suing to seize your public land is not a coincidence — it’s a tell.
And tell every conservation organization, every outdoor recreation company, every hunting and fishing group, every single person who has ever set foot on a national forest and felt something — tell them the time for polite statements and “concern” is over. The building is on fire. The arsonists are inside. And if we don’t act now, there will be very little left to save.
Stay loud. Stay angry. Stay relentless.
They want us tired and resigned. Don’t give them that satisfaction.
These forests belong to you. Fight for them like your life depends on it.
Because it does.
Share
Upgrade to Paid
Thanks for reading. Until next time,
-Jim
Leave a comment


 Melanized C. sphaerospermum. (Rui Tomé/Atlas of Mycology, used with permission)
Melanized C. sphaerospermum. (Rui Tomé/Atlas of Mycology, used with permission)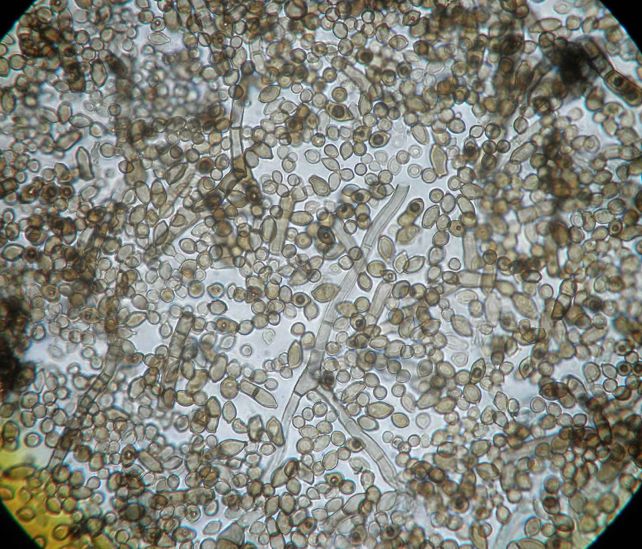 C. sphaerospermum under the microscope. (Rui Tomé/Atlas of Mycology, used with permission)
C. sphaerospermum under the microscope. (Rui Tomé/Atlas of Mycology, used with permission)











.JPG)




.JPG)














.JPG)
.JPG)
.JPG)
.JPG)






.JPG)







{kind=link}